
Delta Variant: Everything You Need to Know

I don’t think people are paying enough attention to Delta, and no single piece I read summarized everything I wanted to know. So here it is. Hope it helps you be more informed and prepared.
Cases are growing exponentially across the world. Again.

If you don’t know where this is going, a historical refresher might help. India has suffered about two million COVID deaths, the majority of them during its latest surge caused by Delta.

And if you think Europe or the US will be spared, this video shows cases in European regions in July 2021 vs. July-November 2020.
Like in the summer of 2020, some areas in the periphery of Europe became hotbeds of cases in July, and after that, cases spread everywhere to form a new wave.
This, mind you, is happening while over 50% of Brits are vaccinated, and 40%+ for the other European countries in the chart.

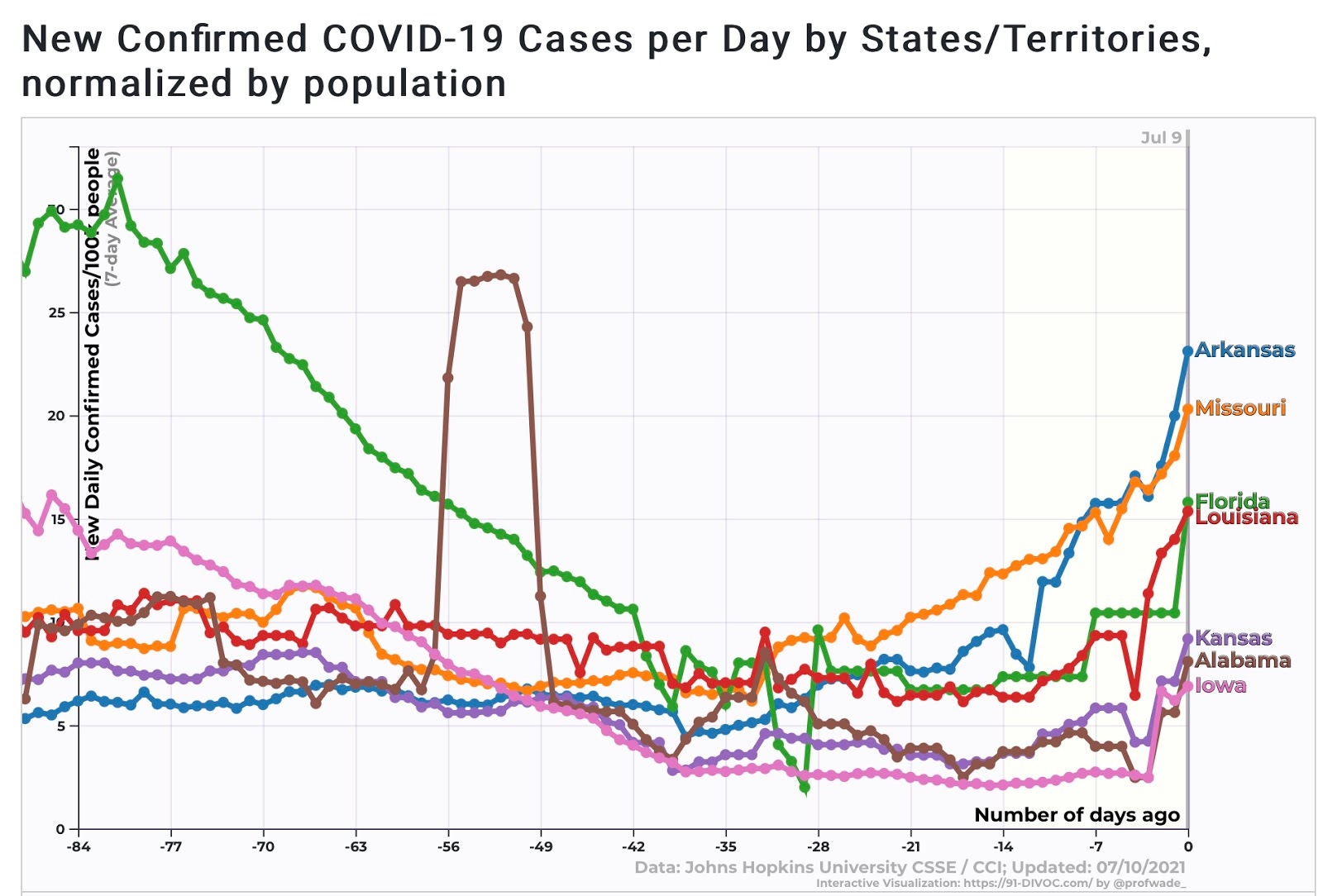
Something similar is happening in the US.
And wherever this is happening, it tends to be Delta. This is what different UK regions are seeing (pink is Delta)

In the UK, it’s the culprit of 99% of cases at the beginning of July 2021. In the US, it’s just ~50%, which means the growth of new cases will still accelerate.
Why is Delta growing so fast? Will it be everywhere as bad as in India? Was this all predictable? What should we do about it?
To answer these questions, we need to start with the fundamentals: the R and fatality rates.
How Bad Is Delta?
Transmissibility
The original Coronavirus variant has an R0 of ~2.71. Alpha—the “English variant” that caused a spike around the world around Christmas—is about 60% more infectious. Now it appears that Delta is about 60% more transmissible yet again. Depending on which figure you use, it would put Delta’s R0 between 4 and 9, which could make it more contagious than smallpox. Just to give you a sense of the dramatic consequence of such an increase in R, this is what two months of growth get you with the previous transmission rate of 2.7 vs. with an R of 6:

This is why so many graphs of cases look like rockets these days. Delta is very contagious.
Apparently, somebody in Australia was infected by the Delta variant just by walking past an infected person, in a 5- to 10- second encounter. Although this is probably an outlier, and we shouldn’t be scared of walking past other people as a rule of thumb, it illustrates how much more transmissible Delta is.

So that’s about transmission rates. What about fatality rates?
Fatality Rates
It looks like the risk of death is 2x higher for Delta than for the original variant:

To put this in context, catching the original COVID approximately doubled your likelihood of death at any age. That means catching Delta approximately triples it.
Why is it deadlier? Weren’t viruses supposed to evolve to be less virulent over time? That’s definitely what people thought before Alpha appeared. I explained why that was unlikely.

Unfortunately, I turned out to be right. The short explanation is that the viruses that tend to win do so because they reproduce faster. Such a virus will grow faster inside a person, and will make that person more infectious, faster. It will also kill that person faster.
With other diseases like Ebola, killing faster means killing too fast to infect many others, so this type of virus doesn’t prevail. Only the ones who at the same time evolve to be less deadly win. But for COVID in our current health system, all the contagions happen early on, much earlier than death. So making death earlier doesn’t matter much.
So is this what’s happening with Delta? Yeah.
One way to tell is the viral load. The higher it is, the more the virus is present. In China, they estimated the viral load of Delta to be 1,000 times higher than that of the original variant.
The most frustrating thing is that this was completely predictable, not just in December, but even in March of 2020.

2.
So Delta, like Alpha before it, is both more transmissible and more fatal. Both of these effects have the same root: the virus is much better at binding to human cells, so it reproduces much faster.
Are people dying more then? Not in Britain.
The Case Fatality Rate (CFR) of Delta there is 0.2%, compared to Alpha’s 1.9%! It’s still early, but it looks like we should already have enough data to tell3. The main reason is probably vaccinations. From Israel:

{kind=link}
The IFR (Infected Fatality Rate4) for the original variant was about 0.01% for those in their 20s and 0.2% for those in their 40s.

With the age of those infected now thanks to the vaccines, of course the new variant will kill fewer people! This is why vaccinations are so important.
How Good Are Vaccines Against Delta?
The best data we have is from Israel, which used Pfizer.
Before Delta, it appeared that full vaccinations reduced infections, hospitalizations, and deaths by 93%, 93%, and 91% respectively. Partial vaccinations were quite good, but not as good.
Now, with Delta, it looks like the figures are 64%, 93% and 93% according to Israel, and 79% for symptomatic infection and 96% hospitalization according to the UK.
That said, Pfizer (and probably Moderna, as similar mRNA vaccines) are likely better than AstraZeneca’s (88% protection against symptomatic infection vs. 60% for AstraZeneca).
That means the protection against hospitalization and death is nearly perfect for mRNA vaccines, but maybe not for infections. How should we interpret this data?
If you’re thinking about yourself, this is very good news. Without vaccination, an 80-year-old might have had a 10% chance of dying from the original COVID and, say, 20% with Delta. Now, with an mRNA vaccine, he has a 2% chance of dying if infected. A 30-year-old might have a 0.02% of dying, much lower than the flu. So get vaccinated as soon as you can.
If you’re a politician, epidemiologist, or social leader, the calculation might be different and depends completely on the type of vaccine in your population, its efficacy, the transmission rate of vaccinated people, and your culture..
First, how many people do you need vaccinated to stop the virus?
Herd Immunity Threshold
If we assume an R0 of 8 and a vaccine effectiveness of 90% against transmission, you need at least 90% of the population vaccinated before you can declare victory. No country is getting close to that.
Consider that mRNA vaccines are only 60% effective against symptomatic infection, and this might be lower for other vaccines. If vaccinated people that end up having symptoms are as infectious as unvaccinated people with symptoms, you end up in a situation where even full vaccination won’t stop the epidemic, and you need a Delta-specific vaccine boost to stop it.
Let’s take an example. Imagine a country that has 50% of its people vaccinated. Imagine the vaccine only reduces infectiousness by 65%. That means R would only have gone down by ~33%5. But Delta’s R is 2-3x higher than the original, so all in all R is now ~50%-100% higher than it was a year ago. These calculations are not precise, but they give you a sense of how much better or worse we will be compared to last year.
Remember, this is the summer in the Northern Hemisphere. Everything is easier now than it will be between September and November.
Long COVID
I haven’t talked about Long COVID yet, but it’s also something to consider. Without vaccines, about 1 in 8 infections will have Long COVID6. That said, if the protection is the same for Long COVID as for infection, hospitalization, or death, Long COVID would go down from ~15% of infections to ~1-4%. It also appears that vaccines can reduce Long COVID afterwards. It is something to keep in mind, but I’m not sure I would change any policy just because of Long COVID at this point. Deaths are enough to quantify the downside.
Takeaways
Delta is a deadly variant. It spreads like wildfire and kills efficiently. We need to be careful.
If you’re an individual
If you’re vaccinated, you’re mostly safe, especially with mRNA vaccines. Keep your guard up for now, avoid events that might become super-spreaders, but you don’t need to worry much more than that.
If you’re not vaccinated though, this is a much more dangerous time than March 2020. The transmission rate is higher than it used to be, and if you catch Delta, you’re much more likely to die—or get Long COVID. You should be extra careful, only hang out with other vaccinated people, and avoid dangerous events.
If you’re a community leader
If you’re in charge of a community, you have two goals:
Vaccinate, vaccinate, vaccinate. The lives of your community depend on it. Any vaccine that works is better than none. If people are opting out, try to lure them in. Most are not anti-vaxxers, but rather they’re on the fence, or simply don’t see the benefit worth the cost. So change their calculation. Create lotteries. The Ohio one, among the first, probably didn’t work, but the cost is paltry compared to the cost of deaths and closing the economy this Fall.
Keep Delta at bay as much as you can while vaccinations proceed. An elimination strategy will be best. Good border fences and test-trace-isolate programs are your best tools. Super-spreader events should still be avoided. Masks indoors and in crowds should be mandatory. Great ventilation is a must.
However, if you have vaccinated everybody that wants to be vaccinated, and the rest simply doesn’t want to get vaccinated, then the calculation changes drastically. If your location values the freedom of its people to make the wrong decisions (as long as they don’t impact others), then you might consider opening up the economy. Delta will tear through those unvaccinated, but that’s their prerogative. Maybe the reality will hit better then.
But it really depends on each society. Opening up without full vaccination would infect some of those vaccinated, about 10% of them would get long COVID7, and about 0.3% of them would die8.
So here each society needs to decide. Say 40% don’t want to vaccinate. Is the freedom of 40% to not vaccinate worth the deaths and Long COVID of those vaccinated? Otherwise, are you willing to force people to vaccinate? Are you going to keep the country closed until there’s a booster vaccine? Will you be able to get your fences and test-trace-isolate programs to work?
If you’re in charge of vaccine policy
An R0 of 8 is bad news for herd immunity. It puts its threshold at ~90% of people protected, which is impossible to reach if vaccines are only 65% protective of infection. Booster shots are necessary. Let’s accelerate their testing, approval, release, and deployment.
Also, support vaccine mix-and-match. In most countries, today, if you need a boost you are forced to take the same vaccine. But mixing types likely protects you better and is as safe as using the same type.
If you’re in a developing country
We don’t pay enough attention to developing countries. Most of the science and media focuses where the money is, in developed economies.
But Delta is very hard in developing countries, especially in dense urban areas where the poor are forced to work but live in close quarters with many others. India, Argentina, Tunisia, South Africa, and Indonesia are very sad examples of this.
Unfortunately, there’s not many special tricks that poor countries can pull. They tend to have a younger population, which helps. The one thing they have going on for them is that they tend to be warmer and more humid, which helps against COVID. Also, thanks to a warmer weather, they can have more events outdoors. This is the one thing they can leverage: have as many of your gatherings outside, while you do everything you can to vaccinate your population, and delay as much as you can the arrival of Delta with strong fences.
Let’s hope vaccine production keeps growing and people the world over can get vaccinated before the fall.
If this piece was relevant to you, share it with those you think it can help.
Meaning each infected person spread it to 2.7 other people. If you go to GitHub and average out all the calculations of R0 for the early variant, you’ll get that 2.7.
The ranges for IFRs were still unclear at that time, hence the quote of millions for countries like the US or the UK. But it wasn’t far off. The US was at 900k deaths by May 2021, and that’s with all the measures taken and the vaccines. And if the virus was let to run wild in the UK, with an R = 6 and an IFR of 2.2%, that would be 1.2M.
Just by comparing with Alpha. Most people die within 28 days of the initial infection, and this should be even faster with Delta. We have about 40 days of Delta data in the UK, so a few people who were infected early should have already had a decisive outcome. Looking at the first 40 days of Alpha, the CFR was above 4%, so 20x higher than for Delta.
Remember, the difference between IFR and CFR is that IFR is the true rate of death, but it’s always estimated, because cases are known, whereas infections are estimated.
Back of the envelope: 50% of vaccinated people * 65% of protection against infectiousness = 33% reduction in infectiousness. These are percentage points
30% of symptomatic cases, but those are only 50% of all cases
~12%*90% vaccine effectiveness
3% IFR * 90% vaccine effectiveness
Chris is 100% wrong. Everything in Thomas Pueyos article is exact and correct,clear and focused. I have called each of the 3 world waves when there was only a few 100 cases.
[In 1st wave, (WILD Strain), thats 100 cases OUTSIDE China. ])
I know he is right.
Another great article Tomas. I think one point is too simplistic; 'Delta will tear through those unvaccinated, but that’s their prerogative'. There are many people that cannot have a vaccine even if they wanted to (eg immunosuppressed, etc), so they basically have to continue hiding away in isolation while the virus rips through society.
As you indeed said, 'If your location values the freedom of its people to make the wrong decisions (as long as they don’t impact others)...' - it DOES impact others. It is certainly unfortunate if you live somewhere the govt and/or populace is making that wrong/foolish decision for you against your will, but that's a separate argument...